Shoulder pain can make everyday activities surprisingly difficult. Reaching overhead, lifting a bag, fastening a seatbelt, getting dressed, or even sleeping comfortably may become painful. While many shoulder conditions improve with rest, physiotherapy, and medications, persistent pain and weakness can sometimes indicate a rotator cuff tear.
A rotator cuff tear is one of the most common causes of shoulder pain in adults. It may develop suddenly after an injury or gradually over time as the tendons naturally weaken with age. However, not every tear requires surgery, and not every painful shoulder is caused by a rotator cuff injury. An accurate diagnosis is essential before deciding the most appropriate treatment.
At Mangal Anand Hospital, Chembur, patients with shoulder injuries are evaluated by orthopaedic surgeons experienced in shoulder arthroscopy, sports injuries, joint preservation, and shoulder reconstruction. Every treatment plan is individualised after carefully assessing your symptoms, shoulder function, clinical examination, imaging findings, lifestyle, and recovery goals.
Whenever clinically appropriate, treatment begins with conservative measures such as physiotherapy, activity modification, medications, PRP therapy, or ultrasound-guided injections. If surgery becomes necessary, minimally invasive arthroscopic techniques are preferred whenever suitable to preserve healthy tissues, restore shoulder function, and support a structured rehabilitation programme.
The shoulder is the most mobile joint in the human body. This remarkable range of movement allows you to lift, throw, reach, push, pull, and rotate your arm in almost every direction. Unlike the hip joint, however, the shoulder sacrifices stability to achieve this flexibility, making it more susceptible to injury.
The rotator cuff plays a critical role in maintaining this balance between movement and stability. It is a group of muscles and tendons that work continuously to keep the shoulder joint centred while allowing smooth, controlled motion. Every time you lift your arm, reach for an object, comb your hair, or place something on a high shelf, the rotator cuff is actively working.
When one or more of these tendons become torn, everyday movements may become painful and difficult. Some patients experience a sudden injury after a fall or sporting activity, while others notice gradually worsening pain over several months due to tendon degeneration. Depending on the severity of the injury, patients may develop pain, weakness, stiffness, difficulty lifting the arm, or disturbed sleep because of shoulder discomfort.
Early assessment is important because a rotator cuff tear can progress over time. Although many patients improve with non-surgical treatment, larger or untreated tears may gradually enlarge, making future treatment more challenging. A timely diagnosis allows your orthopaedic surgeon to recommend the most appropriate treatment based on your individual condition rather than following a standard treatment pathway.
Understanding how the shoulder functions helps explain why a rotator cuff tear can significantly affect both movement and quality of life.
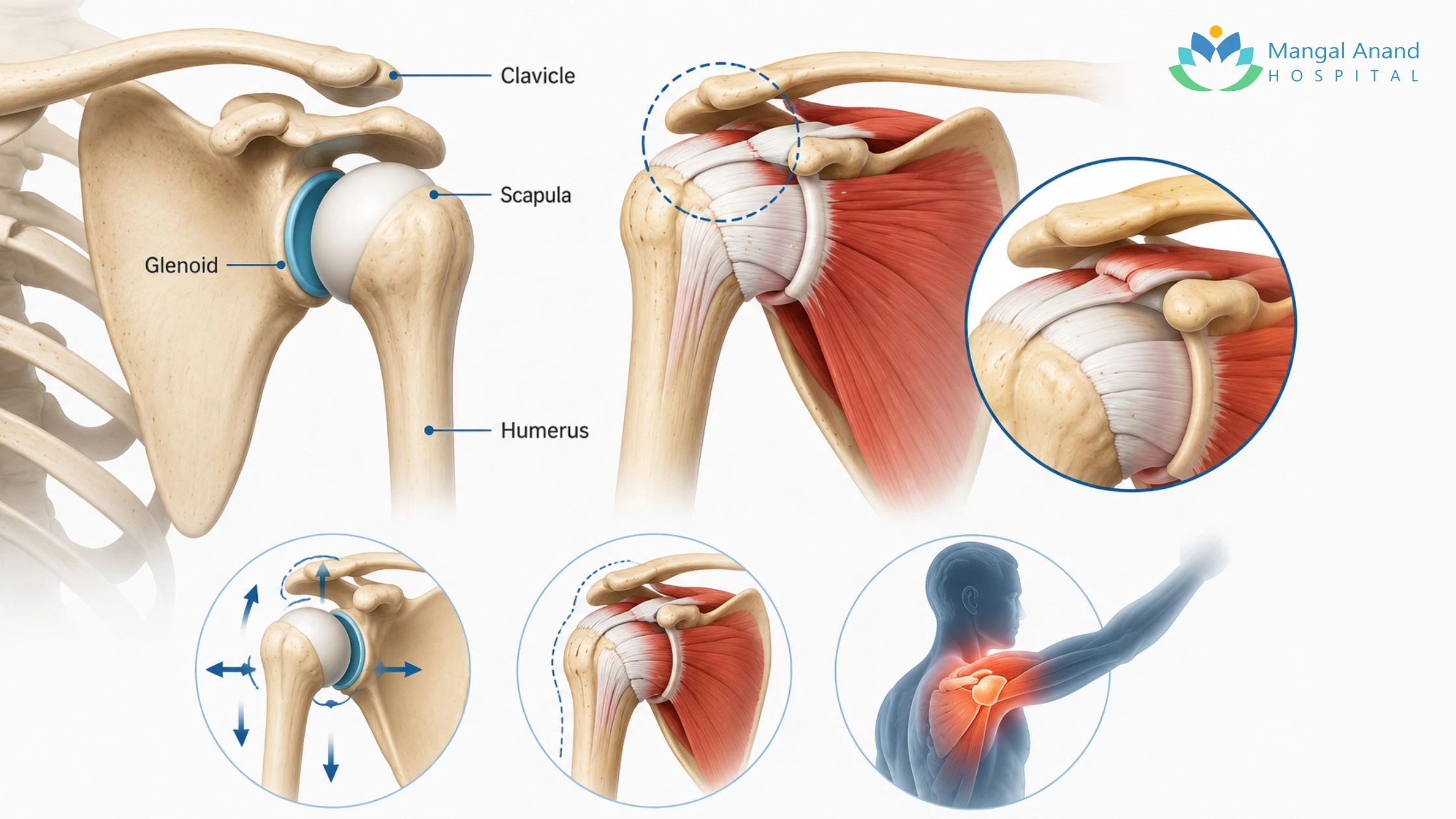
The shoulder is a ball-and-socket joint formed by three bones:
The rounded head of the humerus fits into a shallow socket in the scapula called the glenoid. Because this socket is relatively shallow, the shoulder relies heavily on surrounding muscles, tendons, ligaments, and cartilage for stability rather than the bones alone.
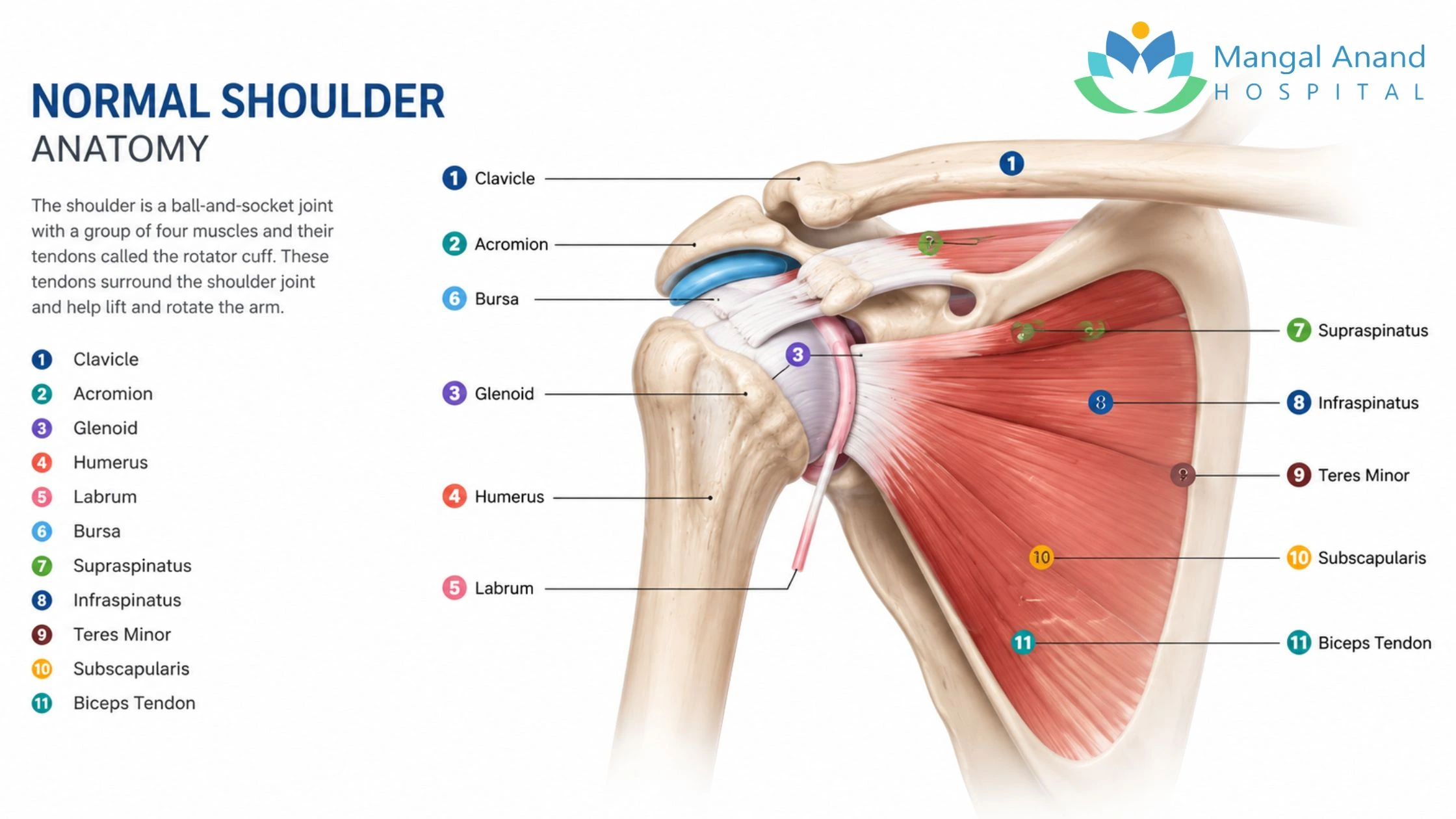
At the centre of this support system is the rotator cuff—a group of four muscles whose tendons surround the shoulder joint. Together, they keep the head of the humerus centred within the socket while allowing smooth, coordinated shoulder movement.
Unlike larger muscles that generate lifting power, the rotator cuff acts as the shoulder's stabilising system. Without it, even simple arm movements become inefficient, painful, and unstable.
Patients with rotator cuff injuries at Mangal Anand Hospital are treated by an experienced orthopaedic team with expertise in shoulder preservation, arthroscopic surgery, sports injuries, trauma, and joint reconstruction.
Dr. Sanjay Singh specialises in shoulder and elbow disorders with advanced fellowship training in Shoulder & Elbow Surgery from Italy. His clinical practice focuses on shoulder arthroscopy, shoulder replacement, sports injuries, and evidence-based rehabilitation, with an emphasis on preserving the native joint whenever possible.

Dr. Nikhil Gokhale completed advanced subspecialty training in the United Kingdom, including a dedicated Shoulder Fellowship at Royal Bournemouth Hospital. His expertise includes arthroscopic shoulder surgery, sports injuries, and complex shoulder reconstruction, supported by extensive clinical experience and ongoing research.

Dr. Pradip Nemade completed his MBBS and MS Orthopaedics from Seth G.S. Medical College & KEM Hospital, followed by DNB Orthopaedics. Since 2009, he has managed complex orthopaedic trauma, shoulder and knee injuries, total hip replacement, and disorders of bones and joints, with a focus on accurate diagnosis, evidence-based treatment, and restoring mobility.

Each muscle performs a specific function, yet all four work together as a single functional unit.
The supraspinatus tendon is the most commonly injured component of the rotator cuff. It initiates lifting the arm away from the body and helps maintain shoulder stability during overhead movements.
Because it passes through a relatively narrow space beneath the acromion, it is particularly vulnerable to wear, repetitive friction, and degeneration over time.
The infraspinatus rotates the arm outward and plays an important role in activities such as reaching behind you, throwing, or placing objects away from your body. It also contributes significantly to shoulder stability during movement.
Although smaller than the other rotator cuff muscles, the teres minor assists with external rotation and works closely with the infraspinatus to maintain balanced shoulder mechanics. Its contribution becomes particularly important during sporting activities and overhead movements.
The subscapularis is the largest and strongest muscle of the rotator cuff. Located at the front of the shoulder blade, it rotates the arm inward and provides stability during pushing, lifting, and reaching activities. It is also essential for maintaining the normal position of the shoulder joint throughout daily movements.
Every shoulder movement depends on a carefully coordinated interaction between muscles, tendons, ligaments, and bones.When you raise your arm, larger muscles such as the deltoid generate the lifting force. At the same time, the rotator cuff continuously keeps the ball of the humerus centred within the shoulder socket. This coordinated action prevents excessive movement of the joint and allows smooth, pain-free shoulder function.
When one of the rotator cuff tendons tears, this balance is disrupted. The shoulder may become painful, weak, and unstable. Patients often notice difficulty performing activities that were previously effortless, including:
The severity of symptoms often depends on the size of the tear, the tendon involved, muscle strength, and the patient's daily activity level.
A rotator cuff tear occurs when one or more of the rotator cuff tendons become partially or completely detached from their attachment on the upper arm bone (humerus). The injury may involve minor fraying of the tendon fibres, a partial-thickness tear, or complete separation of the tendon from the bone.
Rotator cuff tears are among the most common shoulder injuries seen by orthopaedic surgeons. They affect individuals of all ages but become increasingly common after the age of 40 as tendons naturally lose strength, elasticity, and blood supply.
Not every tear develops because of a major injury. Many patients experience gradual tendon degeneration over several years before symptoms become noticeable. Others develop an acute tear after a fall, lifting a heavy object, a shoulder dislocation, or a sporting injury.
Persistent shoulder pain should never be ignored simply because it develops gradually. While not every rotator cuff tear requires surgery, delaying assessment may allow the tendon to retract further, muscles to weaken, and shoulder function to deteriorate.
An early consultation helps determine the underlying cause of your symptoms and identifies whether conservative treatment or surgical intervention is more appropriate. At Mangal Anand Hospital, every patient undergoes a comprehensive evaluation that combines clinical examination with appropriate imaging to understand not only the presence of a tear but also how it is affecting shoulder function.
Timely diagnosis allows treatment to begin before the condition progresses, helping preserve the natural tendon whenever possible, reduce pain, restore movement, and support a safe return to work, sport, and everyday activities.
Not all rotator cuff tears are the same. The size of the tear, the tendon involved, how the injury occurred, and the quality of the surrounding muscles all influence symptoms, treatment options, and recovery.
Some tears develop suddenly after an injury, while others progress gradually over several years. Understanding the type of tear helps your orthopaedic surgeon determine whether conservative treatment is appropriate or whether surgical repair should be considered.
A partial-thickness tear means the tendon has been damaged but is not completely detached from the bone. Instead, only a portion of the tendon fibres are torn.
These tears commonly develop because of gradual tendon degeneration, repetitive overhead activities, or shoulder impingement.
Patients with a partial tear may experience:
Many partial-thickness tears can be managed successfully with non-surgical treatment, particularly when diagnosed early and combined with structured physiotherapy and activity modification.
A full-thickness tear occurs when the tendon completely separates from its attachment on the humerus. Depending on the size of the tear, shoulder strength and function may be significantly affected.
Common symptoms include:
Some patients are unable to raise the arm normally, while others compensate using surrounding muscles. Treatment depends on several factors, including the size of the tear, tendon quality, shoulder function, activity level, and the patient's expectations.
An acute tear develops suddenly following a significant injury.
Common causes include:
Patients often describe a sudden sharp pain followed by weakness and difficulty moving the shoulder.
Early assessment is important because timely treatment may improve the chances of successful tendon repair in appropriate cases.
Degenerative tears develop gradually over time as tendons naturally weaken with age.
Repeated stress on the shoulder can slowly damage the tendon fibres until they eventually tear.
This type of injury is more commonly seen in people who regularly perform repetitive overhead activities, including:
Symptoms often begin gradually and may initially be mistaken for simple shoulder strain. As the tear progresses, patients usually notice increasing pain, weakness, reduced shoulder function, and difficulty performing everyday activities.
As we age, the rotator cuff tendons gradually lose elasticity and receive a reduced blood supply. These natural changes make the tendons more susceptible to small injuries that accumulate over time.
For this reason, rotator cuff tears become increasingly common after the age of 40, even in people who have not experienced a major shoulder injury.
Repeated overhead movements place continuous stress on the rotator cuff.
Over time, these repetitive movements may lead to tendon irritation, inflammation, and eventual tearing.
This is commonly seen in:
Many sports require repetitive shoulder movement at high speed.
Activities such as cricket, tennis, badminton, volleyball, swimming, baseball, and weight training place considerable demands on the rotator cuff.
Sudden forceful movements or repeated overhead actions may result in tendon injury, particularly when shoulder muscles become fatigued.
A healthy tendon can also tear following significant trauma.
Examples include:
These injuries often cause immediate pain, weakness, and reduced shoulder movement.
In some individuals, the rotator cuff repeatedly rubs against the underside of the acromion during shoulder movement. This repeated friction, known as shoulder impingement, can gradually damage the tendon, eventually leading to a partial or complete tear.
Small bony projections, called bone spurs, may develop as part of age-related joint changes.
These spurs can narrow the space available for the rotator cuff tendons, increasing friction during shoulder movement and contributing to tendon wear over time.
The symptoms of a rotator cuff tear vary depending on the size of the tear, the tendon involved, and the patient's activity level.Some patients experience sudden severe pain after an injury, while others notice gradually worsening shoulder discomfort over several months.
Common symptoms include:
Many patients initially notice difficulty performing simple daily activities such as:
Because these symptoms may also occur in conditions such as frozen shoulder, shoulder arthritis, or shoulder impingement syndrome, a detailed clinical evaluation is important to establish the correct diagnosis.
Although anyone can develop a rotator cuff injury, certain factors increase the likelihood of tendon damage.
Risk factors include:
Having one or more risk factors does not necessarily mean a rotator cuff tear will develop, but recognising these factors may help encourage earlier evaluation when symptoms appear.
An accurate diagnosis is the foundation of successful treatment. Shoulder pain alone does not confirm a rotator cuff tear, as several conditions—including frozen shoulder, shoulder impingement syndrome, arthritis, labral injuries, and biceps tendon disorders—can produce similar symptoms.
For this reason, diagnosis is based on a combination of your medical history, clinical examination, shoulder function, and imaging studies rather than relying on a single test or MRI report.
At Mangal Anand Hospital, every patient undergoes a comprehensive assessment to identify not only whether a tendon has torn, but also the size of the tear, the tendons involved, shoulder stability, muscle strength, and the impact on day-to-day function. This comprehensive approach helps ensure that treatment recommendations are tailored to the individual rather than the scan alone.
Your orthopaedic surgeon will begin by understanding how your symptoms developed.
Important questions include:
These answers often provide valuable clues about whether the injury is acute, degenerative, or related to another shoulder condition.
Physical Examination
A detailed shoulder examination helps determine which tendon is affected and whether shoulder weakness is caused by pain, tendon damage, or another underlying condition.
Your surgeon may assess:
The examination also helps differentiate a rotator cuff tear from conditions such as frozen shoulder or shoulder arthritis, which often require different treatment strategies.
Several well-established clinical tests help evaluate the function of individual rotator cuff tendons.
Depending on your symptoms, your surgeon may perform tests such as:
These tests are not used in isolation but are interpreted together with your symptoms and imaging findings to improve diagnostic accuracy.
Imaging studies provide detailed information about the condition of the shoulder joint and surrounding soft tissues.
Although rotator cuff tendons cannot be seen on an X-ray, this investigation helps identify:
X-rays also help rule out other causes of persistent shoulder pain.
Musculoskeletal ultrasound allows dynamic assessment of the rotator cuff while the shoulder is moving.
It can help detect:
Ultrasound is particularly useful in experienced hands and may also be used to guide therapeutic injections with greater precision.
Magnetic Resonance Imaging (MRI) is the most detailed investigation for evaluating rotator cuff injuries.
An MRI helps determine:
These findings help guide treatment planning, particularly when surgery is being considered.
One of the most common misconceptions is that every MRI-confirmed tear requires surgery.
In reality, many people have rotator cuff tears that cause little or no pain, while others experience significant symptoms despite relatively small tears.
Treatment decisions are therefore based on the complete clinical picture, including:
This patient-centred approach helps avoid unnecessary surgery while ensuring that patients who may benefit from surgical repair receive timely treatment.
This is one of the most common questions patients ask after being diagnosed with a rotator cuff tear.
The answer depends on several factors, including the type of tear, its size, symptoms, shoulder function, and your daily activity requirements.
A torn tendon does not typically reattach to the bone on its own. However, many patients experience significant improvement in pain, strength, and shoulder function without surgery, particularly when the tear is small or partial and a structured rehabilitation programme is followed.
The primary goal of non-surgical treatment is to reduce pain, improve shoulder mechanics, strengthen the surrounding muscles, and restore function so that everyday activities become comfortable again.
Treatment recommendations are individualised after carefully evaluating your symptoms, examination findings, and imaging studies.
Whenever clinically appropriate, conservative treatment is usually considered before surgery.
The objective is to relieve pain, improve shoulder movement, restore muscle strength, and help patients return to normal activities without an operation whenever possible.
Continuing painful overhead activities may increase irritation around the injured tendon.
Temporary modification of activities allows inflammation to settle while preventing further stress on the shoulder during the early stages of recovery.Patients are encouraged to remain active while avoiding movements that consistently aggravate symptoms.
Anti-inflammatory medications and pain relievers may help reduce pain and improve comfort during the early stages of treatment. These medications relieve symptoms but do not repair the torn tendon.
They are generally used alongside physiotherapy rather than as a long-term solution.
Physiotherapy is one of the most important components of rotator cuff treatment.
A structured rehabilitation programme focuses on:
Early supervised rehabilitation helps patients regain function safely while reducing the risk of persistent stiffness and muscle weakness.
Platelet-Rich Plasma (PRP) therapy uses a concentrated sample of the patient's own platelets to deliver growth factors into the affected area.In selected patients, PRP may be considered as part of a comprehensive non-surgical treatment plan. The suitability of PRP depends on the nature of the tendon injury, symptoms, clinical findings, and treatment goals.It is not appropriate for every rotator cuff tear and should be recommended only after clinical evaluation.
Image-guided injections allow medication to be delivered accurately to the intended area around the shoulder.Ultrasound guidance improves precision while helping avoid injury to surrounding structures.
Depending on the underlying diagnosis, these injections may be considered to help reduce pain and facilitate rehabilitation.
For active individuals and athletes, rehabilitation extends beyond pain relief.
The programme focuses on:
Recovery plans are individualised according to the patient's sport, functional requirements, and stage of healing.
Not every rotator cuff tear requires surgery, and surgery is not recommended solely because an MRI shows a tendon tear.However, surgical treatment may be considered when non-surgical measures do not provide satisfactory improvement or when the characteristics of the injury suggest that tendon repair may offer better long-term shoulder function.
Depending on the individual clinical situation, surgery may be discussed in patients who have:
The decision is always individualised after carefully reviewing the patient's symptoms, examination findings, imaging studies, occupation, activity level, and treatment goals.Whenever surgery is recommended, your orthopaedic surgeon will explain the expected benefits, potential risks, available surgical options, and rehabilitation process to help you make an informed decision.
When surgery is recommended, arthroscopic rotator cuff repair is the preferred technique for many rotator cuff tears because it allows the tendon to be repaired through small incisions while minimising disruption to surrounding tissues.Using a high-definition arthroscope (a specialised camera), the surgeon visualises the shoulder joint in detail and repairs the torn tendon using specialised instruments and suture anchors. This minimally invasive approach provides excellent visualisation of the joint and allows associated shoulder conditions to be addressed during the same procedure when appropriate.
The choice of surgical technique is individualised and depends on factors such as the size and location of the tear, tendon quality, muscle condition, and overall shoulder function.
Although every procedure is tailored to the individual patient, arthroscopic rotator cuff repair generally involves the following steps:
Clinical Evaluation and Surgical Planning
Before surgery, your orthopaedic surgeon reviews your clinical examination, MRI findings, shoulder function, medical history, and treatment goals to determine the most appropriate surgical approach.
A small camera is introduced through a tiny incision to examine the shoulder joint.
The arthroscope allows detailed evaluation of:
Any additional pathology identified during the procedure can be addressed where appropriate.
The torn tendon is carefully mobilised, while damaged or inflamed tissue may be removed to create an environment that supports tendon healing.The attachment site on the humerus is then prepared to encourage secure tendon healing.
Specialised suture anchors are inserted into the bone.
Strong sutures are then passed through the torn tendon and secured, allowing the tendon to be reattached to its natural position.The repair technique is selected according to the size, pattern, and quality of the tear.
Before completing the procedure, the repair is carefully assessed to ensure appropriate stability and shoulder movement. The small incisions are closed, and the shoulder is placed in a sling to protect the repair during the initial healing phase.
Although arthroscopic repair is appropriate for many patients, it is not the only surgical option.Depending on the condition of the tendon and shoulder joint, your orthopaedic surgeon may recommend an alternative procedure.
Some rotator cuff tears may require a mini-open approach, combining arthroscopy with a small incision to complete the tendon repair.
Large, complex, or revision cases occasionally require open surgery to allow better access to the damaged structures.
In selected patients with irreparable rotator cuff tears, a nearby healthy tendon may be transferred to restore shoulder function.This option is generally reserved for carefully selected cases after detailed clinical evaluation.
When a massive rotator cuff tear is associated with advanced shoulder arthritis and the tendon cannot be repaired, reverse shoulder replacement may provide better pain relief and improved shoulder function.
This procedure changes the mechanics of the shoulder so that the deltoid muscle can compensate for the deficient rotator cuff.
Recovery following rotator cuff repair is a gradual process that extends beyond the operation itself. Successful outcomes depend not only on surgical repair but also on protecting the tendon while it heals and following a structured rehabilitation programme.Every patient's recovery is different, and rehabilitation is individualised according to the type of repair, tendon quality, tissue healing, and functional goals.
Following surgery:
Many arthroscopic rotator cuff repairs can be performed as day-care or short-stay procedures, depending on the patient's overall health and the complexity of surgery.
During the initial healing phase, protecting the repaired tendon is the priority.
Patients are advised to:
As healing progresses, physiotherapy gradually focuses on:
The pace of rehabilitation varies between patients and is adjusted according to healing and clinical progress.
The timeline for returning to work, driving, exercise, and sports varies depending on:
Your surgeon will advise when it is safe to resume different activities rather than following a fixed timetable.
Rotator cuff repair is a well-established procedure with favourable outcomes for appropriately selected patients. However, as with any surgical procedure, complications can occur.
Potential risks include:
Many of these risks can be reduced through careful surgical planning, appropriate rehabilitation, and adherence to post-operative instructions.Before recommending surgery, your orthopaedic surgeon will discuss the expected benefits, potential risks, and available alternatives so that you can make an informed treatment decision.
Although not every rotator cuff tear can be prevented, maintaining good shoulder health may reduce the risk of tendon injury.
Helpful measures include:
Early treatment of shoulder impingement or tendon inflammation may also help prevent progressive tendon damage.
Treatment for a rotator cuff tear should extend beyond repairing a tendon. The objective is to restore shoulder function, relieve pain, preserve healthy tissues whenever possible, and help patients safely return to their daily activities.
At Mangal Anand Hospital, shoulder care is guided by evidence-based orthopaedic practice and individualised treatment planning.
Our approach includes:
Every treatment plan is developed with the aim of helping patients regain comfortable shoulder movement while supporting long-term joint health.
A torn tendon does not usually reattach to the bone on its own. However, many patients experience significant improvement with physiotherapy and other non-surgical treatments, depending on the nature of the tear and their symptoms.
No. Treatment depends on clinical examination, symptoms, shoulder function, imaging findings, activity level, and individual goals rather than MRI findings alone.
Diagnosis combines clinical examination with investigations such as X-rays, ultrasound, and MRI to determine the extent of tendon injury and guide treatment.
Recovery varies between individuals. Tendon healing and rehabilitation progress differ according to the size of the tear, the type of repair performed, and adherence to physiotherapy.
Driving should only be resumed after your surgeon confirms that shoulder movement and strength have recovered sufficiently for safe vehicle control.
Yes. Physiotherapy is an important part of recovery and helps restore shoulder movement, strength, and function.
Many patients return to sporting activities following appropriate rehabilitation. The timing depends on healing, shoulder strength, and the specific sport involved.
Although successful repair restores shoulder function in many patients, a repaired tendon can re-tear. Following rehabilitation advice and gradually returning to activities helps reduce this risk.