Highly experienced doctors
Internationally recognized team of doctors with modern equipment & services
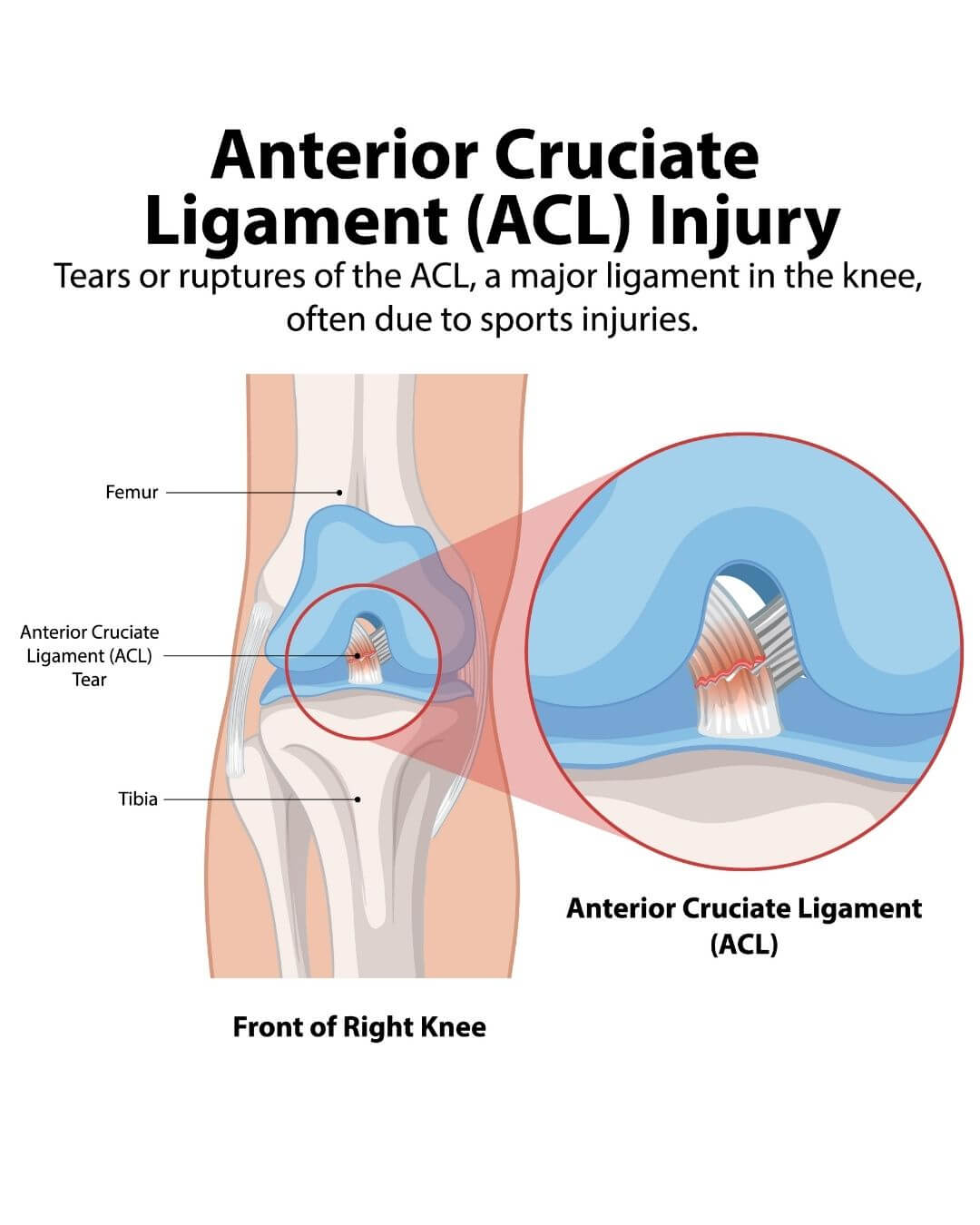
ACL tear treatment is usually considered when the knee becomes unstable after twisting injury, sudden landing, sports trauma, or directional movement that causes swelling, pain, and repeated giving way. Evaluation helps determine whether the ligament is partially injured, completely torn, or associated with meniscus damage that may affect long-term knee stability.
An ACL tear is usually suspected when the knee becomes unstable after a twisting injury, sudden change in direction, awkward landing, or sports-related impact. Many patients seek evaluation when swelling settles after a few days but the knee still feels unreliable during walking, stair climbing, turning, or getting up quickly.
Patients from Chembur, Ghatkopar, Tilak Nagar, Sion, Navi Mumbai, and surrounding parts of Mumbai often consult when they feel that the knee may buckle during movement, especially after football, cricket, badminton, gym injury, running, or accidental twisting.
Not every ACL injury needs surgery. The first step is to understand whether the ligament is partially torn, completely torn, or associated with meniscus damage, cartilage injury, or other ligament involvement.
Most ACL injuries have a very typical early pattern. Many patients describe hearing or feeling a sudden pop at the time of injury, followed by rapid swelling within a few hours.
Common early symptoms include:
sudden knee swelling
pain while putting weight on the leg
difficulty continuing sport or activity
feeling that the knee shifted abnormally
reduced confidence while walking
knee giving way during turning
In some cases, pain reduces after a few days, but instability remains the main complaint. This is often when specialist assessment becomes important.
ACL diagnosis begins with clinical examination. Knee swelling, tenderness, range of movement, and joint stability are assessed before imaging is advised.
A ligament injury cannot be confirmed by pain location alone because some patients continue walking even after a complete tear. ACL assessment specifically checks whether the tibia is moving abnormally relative to the thigh bone.
Clinical examination may include:
Lachman test
anterior drawer test
pivot shift assessment when tolerated
These tests help identify whether the ligament is functioning normally or whether instability is present.
Imaging usually includes:
X-ray to rule out fracture or bony avulsion
MRI to assess ligament tear severity
MRI evaluation for meniscus, cartilage, and associated ligament injury
MRI also helps determine whether the tear is partial, complete, acute, chronic, or associated with other structural damage.
ACL tears often do not occur alone. In many patients, twisting injury also damages the meniscus, which is the cushioning cartilage inside the knee.
In many sports injuries, patients first notice swelling from ACL tear, but locking, catching, or pain while squatting often suggests associated meniscus involvement.
This becomes important because meniscus injury may cause:
locking sensation
sharp pain while squatting
difficulty fully bending the knee
pain during twisting movement
When ACL tear and meniscus injury are present together, treatment planning changes because both stability and joint preservation need attention.
Associated ligament injuries may also involve:
medial collateral ligament
lateral collateral ligament
cartilage surface injury
A partial ACL tear means some ligament fibres remain intact and knee stability may still be partly preserved.
A complete ACL tear means the ligament has lost functional continuity and the knee often becomes mechanically unstable during movement.
Partial tears may present with:
moderate swelling
limited instability
improvement with rehabilitation
Complete tears more often cause:
repeated giving way
difficulty pivoting
instability during sports
fear during quick movement
The treatment approach depends more on knee function than MRI wording alone.
Some ACL injuries can improve without surgery, especially when the tear is partial and knee stability remains acceptable during daily activities.
Non-surgical treatment is often considered when:
instability is minimal
daily walking is comfortable
sports demand is low
no associated major meniscus injury exists
Treatment may include:
swelling control
physiotherapy
muscle strengthening
quadriceps activation
hamstring strengthening
knee brace in selected cases
Many patients first ask whether the ligament can recover naturally. In practice, symptoms improve in some cases, but full mechanical ligament healing is limited in complete tears.
The important question is whether the knee remains stable after rehabilitation.
ACL reconstruction is considered when instability continues despite rehabilitation or when the knee repeatedly gives way during daily movement.
Surgery is more commonly advised when:
the tear is complete
knee buckling continues
sports activity is planned again
meniscus injury is present
more than one ligament is involved
instability affects confidence during daily activity
Young active individuals usually need stronger stability because repeated instability can increase meniscus wear and cartilage damage over time.
The decision is not based only on MRI. It depends on symptoms, examination findings, activity level, and long-term knee demands.

Recovery after ACL injury depends on whether treatment is non-surgical or surgical.
In rehabilitation-only treatment, improvement usually progresses over several weeks depending on swelling control, muscle strength, and knee confidence.
After ACL reconstruction, recovery generally follows phases.
Early phase: first 2 weeks
Focus is on:
swelling reduction
pain control
knee extension
safe walking
Strength phase: 6 weeks to 3 months
Focus shifts to:
quadriceps strengthening
balance control
movement correction
gradual functional loading
Functional recovery phase: 3 to 6 months
Patients work on:
single-leg control
stair confidence
controlled pivot movement
Return to sports phase
Sports return is guided by strength recovery, knee control, and movement testing rather than fixed calendar timelines alone.
Full sports return may take several months depending on healing and rehabilitation quality.
Some patients manage daily life for months after ACL injury, but untreated instability can gradually affect knee health.
Repeated instability may lead to:
meniscus damage
cartilage wear
recurrent swelling
reduced confidence during activity
early joint degeneration
This risk becomes higher when the knee repeatedly twists during routine movement or sports.
The goal of timely treatment is not only pain relief but also protection of long-term knee function.
Many patients understand ACL injury only after swelling improves but instability continues during turning, climbing stairs, or sudden movement. Short expert explanations often help clarify whether rehabilitation is enough or whether ligament reconstruction should be discussed.



ACL treatment often needs accurate decision-making because not every tear behaves the same way.
At Mangal Anand Hospital, treatment planning considers:
With orthopaedic specialists managing ligament injuries, arthroscopy procedures, and joint preservation cases, treatment decisions can be matched more precisely to injury pattern, age, activity level, and future knee demands.
Patients benefit from:
Internationally recognized team of doctors with modern equipment & services
Get all your medical care under one roof with state-of-the-art facilities and equipment
Patient comfort and safety, with a clean and hygienic environment and 24/7 nursing care



Partial tears may improve with rehabilitation if knee stability remains acceptable. Complete tears usually remain mechanically unstable in active individuals.
Yes, many patients can walk after swelling reduces, but instability often appears during turning, stairs, or sudden movement.
Recovery depends on tear severity, treatment type, and rehabilitation quality. Surgical recovery usually takes several months before full sports clearance.
No. Surgery depends on instability, activity demands, associated injury, and functional goals.
Yes. ACL tears frequently occur with meniscus injury, especially after twisting trauma.
Early ACL evaluation often helps clarify whether swelling and instability are settling with rehabilitation or whether ligament reconstruction may be needed to protect long-term knee stability, especially in active patients who want confident movement again.